

Multisystemic Anomalies in Conjoined Twins: The Role of Imaging in Management
Article Sidebar
Views | PDF/EPUB Downloads:
167
/ 19
/ 14
Main Article Content
Abstract
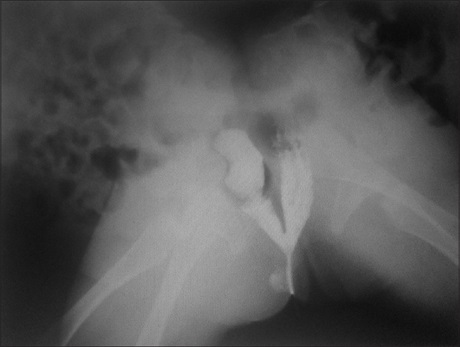
Conjoined twins (CT) represent one of the rarest and most challenging congenital malformations arising as an unfortunate complication of monozygous twinning, with an estimated incidence ranging from 1 in 50,000 to 100,000 pregnancies, with an overall true incidence of about 1 in 200,000 live births with around 60% of them being stillborn. The types of the twins may differ depending on the site of fusion or nonseparation. The most commonly encountered types are thoraco-omphalopagus (28%), thoracopagus (18%), omphalopagus (10%), parasitic twins (10%), pygopagus (6–19%), and craniopagus (6%), with the pygopagus twins having the highest survival rate. Because of the highly variable and complex anatomy and associated malformations, skilled clinical assessments aided by detailed radiological studies, appropriate planning, and teamwork are required for the successful separation of the CT. The role of imaging in the diagnosis and management of missed diagnosed intrauterine case of pygopagus type CT was presented. At delivery, they were found to have sacral fusion on radiography with distal, rectal fusion on limited barium enema. Magnetic resonance imaging demonstrated distal spinal cord fusion with vascular anomaly found on computed tomography angiography. The surgical separation of the patients was successful with satisfactory postoperative lives.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Spitz L, Kiely EM. Experience in the management of conjoined twins. Br J Surg 2002;89:1188‑92.
2. Rode H, Fieggen AG, Brown RA, Cywes S, Davies MR, Hewitson JP, et al. Four decades of conjoined twins at Red Cross Children’s Hospital – Lessons learned. S Afr Med J 2006;96 (9 Pt 2):931‑40.
3. Hirokazu T, Takayuki I, Yoshinori H, Kazunari K, Akio A, Keiji K. Separation surgery of pygopagus asymmetrical conjoined twins sharing U‑shaped spinal cord: Case report and literature review. Childs Nerv Syst 2013;29:699‑706.
4. Jain P, Kundal KA, Sharma R, Khilnani P, Kumar P. Surgical separation of pygopagus twins: A case report. J Pediatr Surg Case
Rep 2014;1:1‑3.
5. Nyundo M, Jahn A, Kayondo K, Ntirenganya F, Muzungu K, Ntakiyiruta G, et al. Successful separation of conjoined pyopagus
twins in African environment with limited resources. Rwanda Med J 2012;69:47‑50.
6. Sun TS, Li SG, Zhang ZC, Li F, Guan K. Preoperative preparation and surgical separation of conjoined pygopagus twins. Chin Med
J (Engl) 2010;123:1800‑3.
7. Weiss JL, Devine PC. False positive diagnosis of conjoined twins in the first trimester. Ultrasound Obstet Gynecol 2002;20:516‑8.
8. Uba AF, Chirdan LB, Yiltok LJ, Ihezue CH, Isamade ES. Management of conjoined twin; a report of two sets. Niger J Surg 2007; 13:20‑4.
9. Anjani J, Kundal K, Sharma R, Khilnani P, Kumar P. A case report. J Pediatr Surg 2014;10:1‑3.
10. Janik JS, Hendrickson RJ, Janik JP, Bensard DD, Partrick DA, Karrer FM. Spectrum of anorectal anomalies in pygopagus twins. J Pediatr Surg 2003;38:608‑12.