

Routine addition of diffusion‑weighted imaging to pediatric brain imaging with acute presentation: An initial experience
Article Sidebar
Views | PDF/EPUB Downloads:
142
/ 54
/ 37
Main Article Content
Abstract
Context: A number of disorders affecting the pediatric brain pose a diagnostic challenge. Magnetic resonance imaging (MRI) is widely accepted as a sensitive technique for the diagnosis of ischemia, encephalitis, and leukodystrophies. Conventional MR sequences used in routine practice include T1-weighted (T1-W), T2-weighted, and fluid-attenuation inversion recovery (FLAIR) sequences. However usually, the presentation in small children is confusing and presents a diagnostic challenge even after the use of these various MR sequences requiring repeated MRI examinations. Detecting pathological changes occurring at microenvironment level is vital for early diagnosis, effective treatment, and obviating the need of repeated MRI.
Aims: The purpose of our study was to assess the additional role of diffusion-weighted imaging (DWI) in better detection of these various pathologies of brain. Settings and Design: This was a prospective study.
Subjects and Methods: Thirty children of ages ranging from neonate to 12 years of age with various complaints of central nervous system involvement were evaluated with MRI brain within 72 h of initial clinical presentation. T1 and T2 spin-echo sequences FLAIR and postcontrast T1-W imaging were done. DWI was performed with echoplanar imaging using depth-resolved surface coil spectroscopy sequence. The lesions were evaluated on DWI and conventional sequences. The final diagnosis was established on the basis of clinical evaluation, electroencephalographic findings, imaging, cerebrospinal fluid analysis, serologic tests, and fatty acid evaluation in plasma assay.
Statistical Analysis Used: This was a descriptive study.
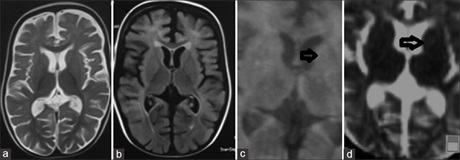
Results: The patients were divided into three groups. Group A included patients in whom DWI detected more lesions or showed a greater extent of lesions on apparent diffusion coefficient (ADC) map than conventional MRI. This group had 11 cases including 7 cases of ischemic encephalopathy, one case of adrenoleukodystrophy (ADL) showing increased extent of lesion with restricted diffusion at the advancing edge and 3 cases of viral encephalitis. In Group B, 12 cases had similar results in both DWI and conventional MRI imaging. Of these, 7 cases with no specific diagnosis and subsequent spontaneous recovery showed no lesion on both conventional and DWI; 5 cases showed equal extent and number of lesions on DWI; 1 case was diagnosed as ADL, 2 as viral encephalitis, and 2 as ischemic encephalopathy on final workup. In Group C, T2 and FLAIR showed more lesions than DWI and had 7 cases. 5 had normal ADC maps but 1–2 small hyperintense lesions on T2 and FLAIR imaging, while the remaining two diagnosed with ischemic encephalopathy had hyperintense areas on T2 and FLAIR sequences with associated ventricular enlargement
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Wedeen VJ, Hagmann P, Tseng WY, Reese TG, Weisskoff RM. Mapping complex tissue architecture with diffusion spectrum magnetic
resonance imaging. Magn Reson Med 2005;54:1377‑86.
2. Sahin T, Bozgeyik Z, Menzilcioglu MS, Citil S, Erbay MF. Importance of Diffusion weighted magnetic resonance imaging in evaluation of
the treatment efficacy in multiple sclerosis patients with acute attacks. Pol J Radiol 2015;80:544‑8.
3. Van der Knaap MS, Valk J. Magnetic Resonance of Myelination and Myelin Disorders. 3rd ed. Berlin: Springer; 2005. p. 141‑3.
4. Tuch DS, Reese TG, Wiegell MR, Wedeen VJ. Diffusion MRI of complex neural architecture. Neuron 2003;40:885‑95.
5. Kamran S, Bener AB, Alper D, Bakshi R. Role of fluid‑attenuated inversion recovery in the diagnosis of meningitis: Comparison with
contrast‑enhanced magnetic resonance imaging. J Comput Assist Tomogr 2004;28:68‑72.
6. Rutherford M, Counsell S, Allsop J, Boardman J, Kapellou O, Larkman D, et al. Diffusion‑weighted magnetic resonance imaging in term perinatal brain injury: A comparison with site of lesion and time from birth. Pediatrics 2004;114:1004‑14.
7. Prakash M, Kumar S, Gupta RK. Diffusion‑weighted MR imaging in Japanese encephalitis. J Comput Assist Tomogr 2004;28:756‑61.
8. Bajaj M, Mody S, Natarajan G. Clinical and neuroimaging findings in neonatal herpes simplex virus infection. J Pediatr 2014;165:404‑7.e1.
9. McCabe K, Tyler K, Tanabe J. Diffusion‑weighted MRI abnormalities as a clue to the diagnosis of herpes simplex encephalitis. Neurology
2003;61:1015‑6.
10. Bladowska J, Kulej D, Biel A, Zimny A, Kalwak K, Owoc‑Lempach J, et al. The role of MR imaging in the assessment of clinical outcomes in children with X‑linked adrenoleukodystrophy after allogeneic haematopoietic stem cell transplantation. Pol J Radiol 2015;80:181‑90.
11. Soares BP, Provenzale JM. Imaging of Herpesvirus Infections of the CNS. AJR Am J Roentgenol 2016;206:39‑48.
12. Küker W, Nägele T, Schmidt F, Heckl S, Herrlinger U. Diffusion‑weighted MRI in herpes simplex encephalitis: A report of three cases.
Neuroradiology 2004;46:122‑5.
13. Hafezi W, Hoerr V. In vivo visualization of encephalitic lesions in herpes simplex virus type 1 (HSV‑1) infected mice by magnetic resonance
imaging (MRI). Methods Mol Biol 2013;1064:253‑65.
14. Jain R, Deveikis J, Hickenbottom S, Mukherji SK. Varicella‑zoster vasculitis presenting with intracranial hemorrhage. AJNR Am J Neuroradiol 2003;24:971‑4.