

Magnetic resonance imaging of congenital unilateral hypoplasia of the face
Article Sidebar
Views | PDF/EPUB Downloads:
213
/ 50
/ 39
Main Article Content
Abstract
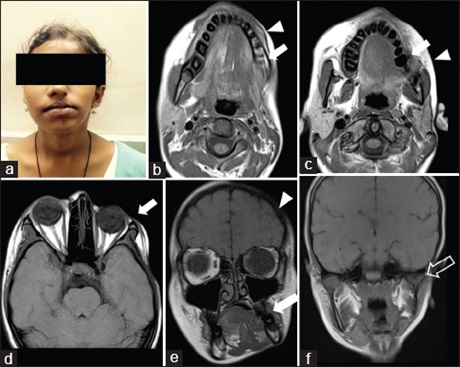
Facial asymmetry may originate from abnormalities of facial musculature, facial innervation, Lateral facial dysplasias or otomandibular dysostosis. We describe Magnetic Resonance Imaging findings of congenital unilateral hypoplasia in a teenager. Case Report: A 15 Year old female referred from plastic surgery department for assessment of congenital unilateral asymmetry of face. Data included relevant history and physical examination and the basic diagnostic work up. The child presented with hypoplastic appearance of facial features on the left side compared to the right side. Asymmetry was more pronounced when she smiled and cried. On examination, the face appeared asymmetric at rest. The left hemiface appeared smaller and showed diffuse deficiency of soft tissue compared to the right side. However the overlying skin appeared normal. No neurological deficit was found in nervous system examination. Magnetic resonance imaging findings revealed diffuse reduction of the subcutaneous fat and muscle tissue on the left side. The left orbital, nasal, maxillary,
mandibular bones showed hypoplasia. Muscle bulk was reduced on the left side with smaller submandibular and parotid salivary glands. Conclusions: Congenital unilateral hypoplasia of face is a rare anomaly that causes asymmetric of face. Pediatricians and otolaryngologists need to be cognizant of cardiac, head and neck, and central nervous system anomalies associated with congenital unilateral hypoplasia of face. The objective of the treatment is to restore facial symmetry and proper function. Teamwork is essential with a board of members including plastic surgeon, otolaryngologist, orthodontist and prosthodontist.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Gorlin RJ, Pindborg JJ. Syndromes of the Head and Neck. New York: McGraw‑Hill; 1976. p. 261‑5.
2. KapurR, KapurR, Sheikh S, Jindal S, Kulkarni S. Hemifacial microsomia: A case report. J Indian Soc Pedod Prev Dent 2008;26 Suppl 1:S34‑40.
3. Romsee MC, Verdonck A, Schoenaers J, et al. Treatment of hemifacial microsomia in a growing child: The importance of co-operation between the orthodontist and the maxillofacial surgeon. J Orthod. 2004;31:190-200.
4. Pruzansky S. Not all dwarfed mandibles are alike. Birth Defects 1969;5:120.
5. Kaban LB, Padwa BL, Mulliken JB. Surgical correction of mandibular hypoplasia in hemifacial microsomia: The case for treatment in early childhood. J Oral Maxillofac Surg 1998;56:628‑38.
6. Vento AR, LaBrie RA, Mulliken JB. The O.M.E.N.S. classification of hemifacial microsomia. Cleft Palate Craniofac J 1991;28:68‑76.
7. Katsanis SH, Jabs EW. Treacher Collins Syndrome. 2004. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, et al. editors. GeneReviews. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1532/PubMed PMID: 20301704. [Last updated on 2012 Aug 30].
8. Gaurkar SP, Gupta KD, Parmar KS, Shah BJ. Goldenhar syndrome: A report of 3 cases. Indian J Dermatol 2013;58:244.
9. Touliatou V, Fryssira H, Mavrou A, Kanavakis E, Kitsiou‑Tzeli S. Clinical manifestations in 17 Greek patients with Goldenhar syndrome. Genet Couns 2006;17:359‑70.
10. Murray JE, Kaban LB, Mulliken JB. Analysis and treatment of hemifacial microsomia. Plast Reconstr Surg 1984;74:186‑99.