

Clinical neonatal hypoxic ischemic injury: Cranial ultrasound spectrum of findings in neonates admitted to a Newborn Unit in Nairobi, Kenya
Article Sidebar
Views | PDF/EPUB Downloads:
860
/ 103
/ 50
Main Article Content
Abstract
Introduction: Birth asphyxia causes significant neurologic injury and neurodevelopmental delay in children. Cranial ultrasound (CUS) can be used for the diagnosis, early intervention, and prognostication of birth asphyxia. We determined the CUS findings among term neonates with clinical birth asphyxia and correlated sonographic findings with the modified Sarnat clinical grade.
Materials and Methods: We conducted a prospective cross-sectional analytical study in Kenyatta National Hospital New Born Unit (KNH NBU) between June 2018 and October 2018. Term babies, older than 24 h with clinical birth asphyxia, were recruited and CUS was performed. Statistical analysis was done using proportions, means, and frequencies. Chi-square tests were used to assess correlation between imaging findings and the clinical Sarnat grading of asphyxia.
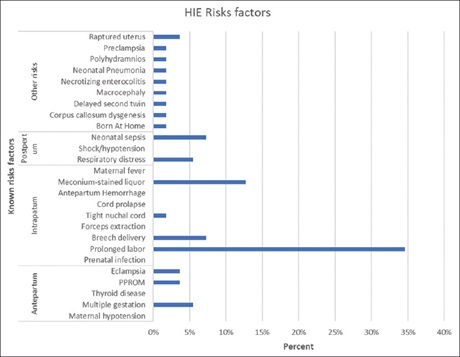
Results: Periventricular deep white matter echogenicity and thalamus and/or basal ganglia deep gray matter was reported in 56.4% and 31.1%, respectively. Only 4.4% had cortical gray matter. Normal CUS findings were reported in 40.0% of the neonates. Prolonged labor and meconium-stained liquor were the predominant risk factors for perinatal asphyxia, seen in 58% of the neonates. Prolonged labor was independently reported in 43% of the neonates. Moderate and severe Sarnat grades correlated with abnormal sonographic changes
of hypoxic ischemic encephalopathy (HIE) (Grades 2–8) (P = 0.038). There was a trend toward HIE severity with worsening Sarnat stages (trend test P = 0.039). Abnormal resistive indices (<0.5 and >0.8) were strongly associated with the presence of HIE brain changes (P = 0.003).
Conclusion: The correlation between birth asphyxia severity and CUS was more robust in Doppler evaluation of the deep cerebral arteries.
Downloads
Article Details
Section
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Marlow N, Budge H. Prevalence, causes, and outcome at 2 years of age of newborn encephalopathy. Arch Dis Child Fetal Neonatal Ed 2005; 90:F193‑4.
2. Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, Bassani DG, et al. Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet 2010;375:1969‑87.
3. Perlman JM. Summary proceedings from the neurology group on hypoxic‑ischemic encephalopathy. Pediatrics 2006;117:S28‑33.
4. Lindström K, Hallberg B, Blennow M, Wolff K, Fernell E, Westgren M. Moderate neonatal encephalopathy: Pre‑ and perinatal risk factors and long‑term outcome. Acta Obstet Gynecol Scand 2008;87:503‑9.
5. Van Bel F, Shadid M, Moison RM, Dorrepaal CA, Fontijn J, Monteiro L, et al. Effect of allopurinol on postasphyxial free radical formation, cerebral hemodynamics, and electrical brain activity. Pediatrics 1998;101:185‑93.
6. Robertson NJ, Edwards AD. Recent advances in developing neuroprotective strategies for perinatal asphyxia. Curr Opin Pediatr 1998;10:575‑80.
7. Epelman M, Daneman A, Kellenberger CJ, Aziz A, Konen O, Moineddin R, et al. Neonatal encephalopathy: A prospective comparison of head US and MRI. Pediatr Radiol 2010;40:1640‑50.
8. Lowe LH, Bailey Z. State‑of‑the‑art cranial sonography: Part 1, modern techniques and image interpretation. AJR Am J Roentgenol 2011; 196: 1028‑33.
9. Ilves P, Lintrop M, Talvik I, Muug K, Maipuu L, Metsvaht T. Low cerebral blood flow velocity and head circumference in infants with severe hypoxic ischemic encephalopathy and poor outcome. Acta Paediatr 2009;98:459‑65.
10. Ghei SK, Zan E, Nathan JE, Choudhri A, Tekes A, Huisman TA, et al. MR imaging of hypoxic‑ischemic injury in term neonates: Pearls and pitfalls. Radiographics 2014;34:1047‑61.
11. Barkovich AJ. Magnetic resonance techniques in the assessment of myelin and myelination. J Inherit Metab Dis 2005;28:311‑43.
12. Johnston MV, Trescher WH, Ishida A, Nakajima W. Neurobiology of hypoxic‑ischemic injury in the developing brain. Pediatr Res 2001; 49: 735‑41.
13. Chao CP, Zaleski CG and Patton AC. Neonatal hypoxic‑ischemic encephalopathy: Multimodality imaging findings. Radiographics: A review publication of the Radiological Society of North America, Inc 2006;26 Suppl 1:S159‑172.
14. Tann CJ, Nakakeeto M, Hagmann C, Webb EL, Nyombi N, Namiiro F, et al. Early cranial ultrasound findings among infants with neonatal
encephalopathy in Uganda: An observational study. Pediatr Res 2016;80:190‑6.
15. Ugwu GI, Abedi HO, Ugwu EN. Incidence of birth asphyxia as seen in central hospital and GN children’s clinic both in Warri Niger Delta
of Nigeria: An eight year retrospective review. Glob J Health Sci 2012;4:140‑6.
16. Palsdottir K, Dagbjartsson A, Thorkelsson T, Hardardottir H. [Birth asphyxia and hypoxic ischemic encephalopathy, incidence and obstetric risk factors]. Laeknabladid 2007;93:595‑601.
17. Kudrevičienė A, Basevičius A, Lukoševičius S, Laurynaitienė J, Marmienė V, Nedzelskienė I, et al. The value of ultrasonography and Doppler sonography in prognosticating long‑term outcomes among full‑term newborns with perinatal asphyxia. Medicina (Kaunas) 2014;50:100‑10.
18. Vannucci RC, Vannucci SJ. Perinatal hypoxic‑ischemic brain damage: Evolution of an animal model. Dev Neurosci 2005;27:81‑6.
19. Biostatistics WD. A Foundation for Analysis in the Health Sciences. 7 ed. Wayne W. Daniel, Wiley, 1999. Stat Med 2001;20:324–6. Doi:
10.1002/1097‑0258(20010130)20:2<324::AID‑SIM635>3.0.CO;2‑O.
20. Martinez‑Biarge M, Diez‑Sebastian J, Kapellou O, Gindner D, Allsop JM, Rutherford MA, et al. Predicting motor outcome and death in term hypoxic‑ischemic encephalopathy. Neurology 2011;76:2055‑61.
21. Barseem NF, Badr HS, Abdullah MS. Color Doppler ultrasonography in full term neonates with hypoxic ischemic encephalopathy and
prediction of outcome. Gaz Egypt Paediatr Assoc 2016;64:38‑43.
22. Mwakyusa SD, Manji KP, Massawe AW. The hypoxic ischaemic encephalopathy score in predicting neurodevelopmental outcomes among infants with birth asphyxia at the Muhimbili National Hospital, Dar‑es‑Salaam, Tanzania. J Trop Pediatr 2009;55:8‑14.
23. Susmita G, Tapan KJ, Arunabha T. Ultrasonographic evaluation of the neonatal Brain in Cases of Birth Asphyxia. Int J Anatomy Radiol Surg 2016;5:58‑63.
24. Ferriero DM. Neonatal brain injury. N Engl J Med 2004;351:1985‑95.
25. Liu J, Cao HY, Huang XH, Wang Q. The pattern and early diagnostic value of Doppler ultrasound for neonatal hypoxic‑ischemic encephalopathy. J Trop Pediatr 2007;53:351‑4.
26. Kirimi E, Tuncer O, Atas B, Sakarya ME, Ceylan A. Clinical value of color Doppler ultrasonography measurements of full‑term newborns with perinatal asphyxia and hypoxic ischemic encephalopathy in the first 12 hours of life and long‑term prognosis. Tohoku J Exp Med 2002;197:27‑33.
27. Shalak L, Perlman JM. Hypoxic‑ischemic brain injury in the term infant‑current concepts. Early Hum Dev 2004;80:125‑41.