

Acute toxicity to radical combination treatment in human immunodeficiency virus‑positive cervical cancer patients: Experience from a resource‑constrained center
Article Sidebar
Views | PDF/EPUB Downloads:
459
/ 114
/ 40
Main Article Content
Abstract
Background and Purpose: To determine acute toxicity to radical combination treatment in invasive cervical cancer patients seropositive to human immunodeficiency virus (HIV).
Subjects and Methods: This is a retrospective review of HIV-seropositive patients managed for invasive cervical cancer between January 2012 and December 2017 at the radiotherapy and oncology center of our institution. Patients’ sociodemographics, disease characteristics, and acute treatment-induced toxicity were extracted from their clinical case notes and were studied.
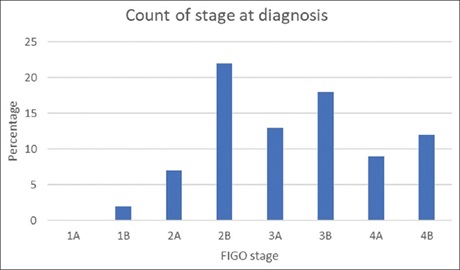
Results: A total of 83 confirmed HIV patients with histologically diagnosed invasive cervical cancer were studied. Their median age at presentation was 37.8 years. The most common presenting symptom of cervical cancer was copious foul-smelling vaginal discharge accounting for 39.8%. Sixty-three (85.6%) patients presented with Eastern Cooperative Oncology Group performance status of 0 and 2 and 74 (89.2%) patients presented with International Federation of Gynecologists and Obstetricians Stage 2B and above. Seventy-four (89.2%) patients had access to highly active antiretroviral therapy. Fifty-five (66.3%) patients were started on radical chemoradiation of which 28 (50.1%) completed prescribed external beam radiotherapy. Thirteen (15.7%) patients were treated symptomatically to control symptoms of cervical cancer. Concurrent chemoradiation appears to be poorly tolerated with 25 (71.4%) of the patients in this arm of treatment developing either Grade 3 or 4 toxicities. Grade 3 hematologic and gastrointestinal tract (GIT) toxicity was seen in 17.9% and 25% of the patients, respectively, while 21.4% of the patients presented with Grade 4 skin toxicity, leading to treatment delays and interruptions. There was excellent symptomatic relief in patients treated with palliative intent.
Conclusions: Radiotherapy and chemotherapy are effective modalities of treatment in a selected group of these set of patients with good control of symptoms related to cervical cancer. Palliative radiotherapy is also effective in patients with poor performance status in relieving symptoms of cervical cancer. Further research needed to be done to identify the optimum management of these patients with radiotherapy and/or chemotherapy to reduce treatment-induced toxicity, thereby minimizing treatment interruptions and delays which ultimately will improve their overall outcome.
Downloads
Article Details
Section
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Oguntayo O, Zayyan M, Kolawole A, Adewuyi S, Ismail H,Koledade K. Cancer of the cervix in Zaria, Northern Nigeria. Ecancermedical science 2011; 5:219.
2. Centers for Disease Control. Revised classification system for HIV infection and expanded surveillance case definition for AIDS among
adolescents and adults. Morbid Mortal Wkly Rep 1993;41:1‑9.
3. Ghebre RG, Grover S, Xu MJ, Chuang LT, Simonds H. Cervical cancer control in HIV‑infected women: Past, present and future. Gynecol
Oncol Rep 2017;21:101‑8.
4. Dryden‑Peterson S, Bvochora‑Nsingo M, Suneja G, Efstathiou JA, Grover S, Chiyapo S, et al. HIV infection and survival among women with cervical cancer. J Clin Oncol 2016;34:3749‑57.
5. Maiman M, Fruchter RG, Serur E, Remy JC, Feuer G, Boyce J. Human immunodeficiency virus infection and cervical neoplasia. Gynecol Oncol 1990; 38:377‑82.
6. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394‑424.
7. Umezulike AC, Tabansi SN, Ewunonu HA, Nwana EJ. Epidemiological characteristics of carcinoma of the cervix in the Federal Capital
Territory of Nigeria. Niger J Clin Pract 2007;10:143‑6.
8. Joint United Nations Programme on HIV/AIDS, editor. Report on the Global HIV/AIDS Epidemic 2008. Geneva: Joint United Nations Programme on HIV/AIDS; 2008.
9. Abdus‑Salam A, Ogunnorin O, Abdus‑Salam R. HIV Seroprevalence in Patients with Carcinoma of the Cervix in Ibadan, Nigeria. Ghana
Med J 2008;42:141‑3.
10. Abdullahi A, Mustapha MI, David DA, Ayodeji OT. Human immunodeficiency virus seroprevalence in patients with invasive cervical cancer in Zaria, North‑Western Nigeria. Ann Afr Med 2018;17:17‑21.
11. Holtz DO, Dunton C. Traditional management of invasive cervical cancer. Obstet Gynecol Clin North Am 2002;29:645‑57.
12. Mackall CL. T‑cell immunodeficiency following cytotoxic antineoplastic therapy: A review. Stem Cells 2000;18:10‑8.
13. Shrivastava SK, Engineer R, Rajadhyaksha S, Dinshaw KA. HIV infection and invasive cervical cancers, treatment with radiation therapy: Toxicity and outcome. Radiother Oncol 2005;74:31‑5.
14. Rubinstein PG, Aboulafia DM, Zloza A. Malignancies in HIV/AIDS: From epidemiology to therapeutic challenges. AIDS 2014;28:453‑65.
15. Holcomb K, Maiman M, Dimaio T, Gates J. Rapid progression to invasive cervix cancer in a woman infected with the human
immunodeficiency virus. Obstet Gynecol 1998;91:848‑50.
16. Amit A, Edwards CL, Athey P, Kaplan AL. Extensive subcutaneous metastases from squamous cell carcinoma of the cervix in patient with
HIV. Int J Gynecol Cancer 2001;11:78‑80.
17. Fruchter RG, Maiman M, Sedlis A, Bartley L, Camilien L, Arrastia CD. Multiple recurrences of cervical intraepithelial neoplasia in women with
the human immunodeficiency virus. Obstet Gynecol 1996;87:338‑44.
18. Lomalisa P, Smith T, Guidozzi F. Human immunodeficiency virus infection and invasive cervical cancer in South Africa. Gynecol Oncol
2000; 77:460‑3.
19. Tomadoni AE, Wainstein RC. Cancer in AIDS patients: Experience at a general hospital in the Province of Buenos Aires. Medicina (B Aires)
1998;58:41‑4.
20. Anorlu RI, Orakwue CO, Oyeneyin L, Abudu OO. Late presentation of patients with cervical cancer to a tertiary hospital in Lagos: What is responsible? Eur J Gynaecol Oncol 2004;25:729‑32.
21. Ikechebelu JI, Onyiaorah IV, Ugboaja JO, Anyiam DC, Eleje GU. Clinicopathological analysis of cervical cancer seen in a tertiary health facility in Nnewi, South‑east Nigeria. J Obstet Gynaecol 2010;30:299‑301.
22. Chirenje ZM, Rusakaniko S, Akino V, Mlingo M. A review of cervical cancer patients presenting in Harare and Parirenyatwa Hospitals in 1998. Cent Afr J Med 2000;46:264‑7.
23. Maiman M, Fruchter RG, Guy L, Cuthill S, Levine P, Serur E. Human immunodeficiency virus infection and invasive cervical carcinoma.
Cancer 1993;71:402‑6.
24. Maiman M, Fruchter RG, Clark M, Arrastia CD, Matthews R, Gates EJ. Cervical cancer as an AIDS‑defining illness. Obstet Gynecol 1997;89:76‑80.
25. Sule ST, Mohammed SS. Cervical cancer management in Zaria, Nigeria. Afr J Health Sci 2007;14:149‑53.
26. Simonds HM, Neugut AI, Jacobson JS. HIV status and acute hematologic toxicity among patients with cervix cancer undergoing radical chemoradiation. Int J Gynecol Cancer 2015;25:884‑90.
27. Ferreira MP, Coghill AE, Chaves CB, Bergmann A, Thuler LC, Soares EA, et al. Outcomes of cervical cancer among HIV‑infected and HIV‑uninfected women treated at the Brazilian National Institute of Cancer. AIDS 2017;31:523‑31.
28. Eifel PJ, Winter K, Morris M, Levenback C, Grigsby PW, Cooper J, et al. Pelvic irradiation with concurrent chemotherapy versus pelvic and para‑aortic irradiation for high‑risk cervical cancer: An update of Radiation Therapy Oncology Group Trial (RTOG) 90‑01. J Clin Oncol 2004; 22:872‑80.
29. Koh WJ, Greer BE, Abu‑Rustum NR, Apte SM, Campos SM, Cho KR, et al. Cervical cancer, version 2.2015. J Natl Compr Canc Netw 2015; 13:395‑404.
30. Chuang LT, Temin S, Camacho R, Dueñas‑Gonzalez A, Feldman S, Gultekin M, et al. Management and care of women with invasive cervical
cancer: American Society of Clinical Oncology resource‑stratified clinical practice guideline. J Glob Oncol 2016;2:311‑40.
31. Lohse N, Obel N. Update of survival for persons with HIV infection in Denmark. Ann Intern Med 2016;165:749‑50.
32. Msadabwe S. Randomized Study to Compare Radical Concurrent Chemoradiotherapy against Radical Radiotherapy, as Treatment of
Cancer of the Cervix in HIV Infected Patients. M.Sc. Diss., University of Witwatersrand, Johannesburg, South Africa; 2009. Available
from: http://wiredspace.wits.ac.za/bitstream/handle/10539/7468/MMed%20R. [Last accessed on 2018 Oct 28].
33. Shiels MS, Cole SR, Kirk GD, Poole C. A meta‑analysis of the incidence of non‑AIDS cancers in HIV‑infected individuals. J Acquir Immune Defic Syndr 2009;52:611‑22.
34. Powles T, Imami N, Nelson M, Gazzard BG, Bower M. Effects of combination chemotherapy and highly active antiretroviral therapy on immune parameters in HIV‑1 associated lymphoma. AIDS 2002; 16:531‑6.
35. Formenti SC, Chak L, Gill P, Buess EM, Hill CK. Increased radiosensitivity of normal tissue fibroblasts in patients with acquired immunodeficiency syndrome (AIDS) and with Kaposi’s sarcoma. Int J Radiat Biol 1995;68:411‑2.
36. Vallis KA. Glutathione deficiency and radiosensitivity in AIDS patients. Lancet 1991;337:918‑9.
37. Kirwan JM, Symonds P, Green JA, Tierney J, Collingwood M, Williams CJ. A systematic review of acute and late toxicity of concomitant chemoradiation for cervical cancer. Radiother Oncol 2003; 68:217‑26.