

Echocardiographic Study of Left Ventricular Function in HIV‑Infected Nigerians
Article Sidebar
Views | PDF/EPUB Downloads:
290
/ 70
/ 43
Main Article Content
Abstract
Context: Left ventricular function in HIV/AIDS patients from South-East Nigeria has not been reported.
Aims: We sought to determine the prevalence and spectrum of left ventricular function abnormalities in patients with HIV infection in the University of Nigeria Teaching Hospital (UNTH), Enugu, South-East Nigeria.
Settings and Design: This was a descriptive, cross-sectional study of patients with HIV/ AIDS at UNTH, Enugu from September 2006 to July 2007.
Methods and Material: Sixty-six HIV-infected patients being managed at the antiretroviral therapy clinic and who had no other cardiovascular risk factor other than HIV infection were consecutively recruited. They were matched for sex, and age with seronegative healthy controls. Clinical and echocardiographic evaluation was carried out to assess the left ventricular function.
Statistical Analysis Used: The findings were analyzed with statistical package for social sciences (SPSS) version 10.0.
Results: The patients consisted of 29 males and 37 females aged between 23 and 62 years. Left ventricular systolic dysfunction was identified in 9 (13.6%) of 66 HIV-infected patients and 1 (4.3%) of 23 controls (P = 0.201) while left ventricular
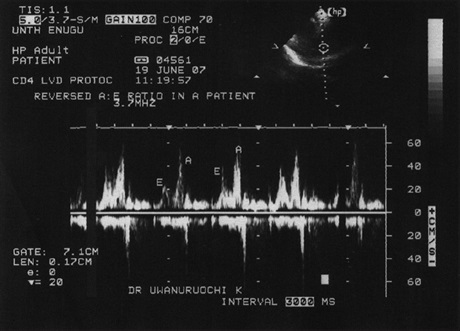
diastolic dysfunction (reversed fi lling pattern) was identifi ed in 19 (28.8%) and 3 (13.0%) of the HIV-infected patients and controls, respectively (0.021). Left ventricular hypertrophy was seen in 2 (3.0%) patients but in only 1 (4.3%) control (P = 0.647), while left ventricular dilatation was absent in all the patients and controls.
Conclusions: Systolic function does not vary significantly between our patients with HIV/AIDS and sero-negative controls. This calls for further investigation of cardiac function in Nigerian HIV/AIDS patients.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Austran B, Gorin I, Leibowitch M, Laroche L, Escande JP, Hewitt J, et al. AIDS in a Haitian woman with cardiac Kaposi’s sarcoma and
Whipple disease. Lancet 1983;1:767‑8.
2. Barbaro G. Cardiovascular Manifestations of HIV infection. J R Soc Med 2001;94:384‑90.
3. Rerkpattanapipat P, Wongpraparut N, Jacobs LE, Kotler MN. Cardiac manifestations of acquired immunodeficiency syndrome.
Arch Intern Med 2000;160:602‑8.
4. Okeahialam BN, Anjorin FL. Echocardiographic study of the heart in AIDS. The Jos experience. Trop Card 2000;26:3‑6.
5. Ige OO, Oguche S, Bode‑Thomas F. Left ventricular systolic function in Nigerian children with human immunodeficiency virus
infection. Congenit Heart Dis 2012;7:417‑22.
6. Olusegun‑Joseph DA, Ajuluchukwu JN, Okany CC, Mbakwem AC, Oke DA, Okubadejo NU. Echocardiographic patterns in treatment‑naïve HIV‑positive patients in Lagos, south‑west Nigeria. Cardiovasc J Afr 2012;23:e1‑6.
7. Godsent I, Basil O, Solomon D, Augustin O, Michael I. Determinants of HIV‑related cardiac disease among adults in north central
Nigeria. Heart Asia 2013;5:130‑5.
8. Araoye MO. Reseach Methodology with statistics for health and social sciences. First Edition. Ilorin: Nathadex Publishers; 2003.
p. 117‑21.
9. Sani MU. Electrocardiographic pattern of patients with AIDS in JUTH, Jos. FMCP Part 2 Dissertation, West African College of
Physicians; 2002.
10. Danbauchi SS, Sani BG, Alhassan AM, Oyati AI. Echocardiographic features of HIV/AIDS subjects on 1‑2 years of ARV drugs in Nigeria. Available from: http://www2.umdnj.edu/shindler/hivecho.html. [Last accessed on 2014 Oct 17].
11. Henry WL, De Maria A, Gramiak R, King DL, Kisslo JA, Popp RL, et al. Report of the American Society of Echocardiography Committee on Nomenclature and standards in 2‑D Echocardiography. Circulation 1980;62:212‑7.
12. Adebiyi AA, Ogah OS, Aje A, Ojji DB, Adebayo AK, Oladapo OO, et al. Echocardiographic partition values and prevalence of left
ventricular hypertrophy in hypertensive Nigerians. BMC Med Imaging 2006;6:10.
13. Report of the WHO/ISFC task force on the definition and classification of cardiomyopathies. Br Heart J 1980;44:672‑3.
14. Vasan RS, Levy D. Defining diastolic heart failure: A call for standardized diagnostic criteria. Circulation 2000;101:2118‑21.
15. Danbauchi SS, Sani SG, Alhassan MA, Oyati AI. Cardiac manifestations of stage III/IV HIV/AIDS compared to subjects on ARV in Zaria, Nigeria. Nig J Cardiol 2006;3:5‑10.
16. Cardoso JS, Moura B, Martins L, Mota‑Miranda A, Rocha Gonçalves F, Lecour H. Left ventriular dysfunction in HIV‑infected
patients. Int J Cardiol 1998;63:37‑45.
17. Longo‑Mbenza B, Tonduangu K, Muvova D, Phuati MB, Seghers KV, Kestelot H. A clinical study of cardiac manifestations related to acquired immunodeficiency syndrome (AIDS) in Kinsaha. Arch Mal Couer Vaiss 1995;88:1437‑43.
18. Longo‑Mbenza B, Seghers LV, Vita EK, Tonduangu K, Bayekula M. Assessment of ventricular diastolic function in AIDS patients from Congo: A Doppler echocardiographic study. Heart 1998;80:184‑9.
19. Yalçin F, Thomas J. Diastolic dysfunction: Pathogenesis, therapy and the importance of doppler echocardiography. Tr J Med Sci
1999;29:501‑5.
20. Lipshultz SE, Chanock S, Sanders SP, Colan SD, Perez‑Atayde A, McIntosh K. Cardiovascular manifestations of HIV infection in
infants and children. Am J Cardiol 1989;63:1489‑97.
21. Herskowitz A, Vlahov D, Willoughby S, Chaisson RE, Schulman SP, Neumann DA, et al. Prevalence and incidence of left ventricular
dysfunction in patients with HIV infection. Am J Cardiol 1993;71:955‑8.
22. Levy WS, Simon GL, Rio SJ, Ross AM. Prevalence of cardiac abnormalities in HIV infection. Am J Cardiol 1989;63:86‑9.