

Role of Computerized Tomography Scan in Seizure Disorders
Article Sidebar
Views | PDF/EPUB Downloads:
363
/ 47
/ 42
Main Article Content
Abstract
Background: Neuroimaging can help to determine whether a seizure in a patient results from a structural abnormality of the brain or its surroundings. It is useful in a variety of clinical settings. The present study was undertaken to find the role of computed tomography (CT) scan in patients of seizure disorders.
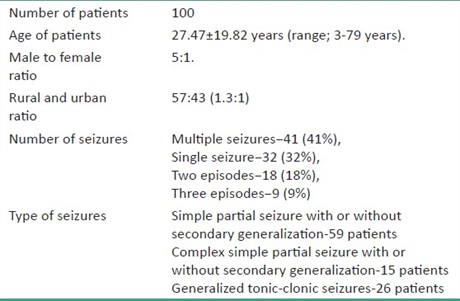
Materials and Methods: This was a prospective study of 2 years duration. The sample size was 100. Nonenhanced CT (NECT) scan was performed in all patients on single slice helical CT scanner. All patients with history of seizures were included in the study. Any patient with evidence of biochemical or metabolic abnormality was excluded.
Results: The mean age of patients was 27.47 ± 19.82 years. The sensitivity of NECT was 49%. Following contrast-enhanced CT (CECT) study, the overall sensitivity came to be 51%. Also, the scans in which NECT was unable to provide a conclusive diagnosis, CECT provided a confirmatory diagnosis in most of them (34 patients, 69.38% of 49 patients). Space-occupying lesions were the most common finding and were more commonly associated with simple seizures with or without generalization.
Conclusion: CT scan plays a very important role as a preliminary tool in radiological assessment of patients presenting with seizure. In about half of the seizure patients, it is able to diagnose or suggest the abnormality. It is valuable in making a diagnosis particulary in Indian subcontinent, where infective causes in form of space occupying lesions and infections are most important cause of seizure.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Hess CP, Barkovich JA. Seizures: Emergency neuroimaging. Neuroimag Clin N Am 2010;20:619‑37.
2. Bernal B, Altman NR. Evidence‑based medicine: Neuroimaging of seizures. Neuroimag Clin N Am 2003;13:211‑24.
3. Huff JS, Morris DL, Kothan RU, Gibbs MA. Emergency Medicine Seizure Study Group. Emergency department management of
patients with seizures: A multicenter study. Acad Emerg Med 2001;8:622‑8.
4. Krumholz A, Grufferman S, Orr ST, Stern BJ. Seizure and seizure care in an emergency department. Epilepsia 1989;30:175‑81.
5. Forsgren L, Bucht G, Eriksson S, Bergmark L. Incidence and clinical characterization of unprovoked seizures in adults: A prospective population‑based study. Epilepsia 1996;37:224‑9.
6. Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota; 1935–1984. Epilepsia
1993;34:453‑68.
7. Rajshekhar V, Haran RP, Prakash S, CHandy MJ. Differentiating solitary small cysticercus granulomas and tuberculomas in patients
presenting with epilepsy: Clinical and computerized tomographic criteria. J Neurosurg 1993;78:402‑7.
8. Rathi V, Thakur LC, Sariwal A. Non contrast‑enhanced four‑detector multisection CT for the detection of ring lesions in seizures. Clin Radiol 2006;61:1041‑6.
9. Nair PP, Kalita J, Misra UK. Role of cranial imaging in epileptic status. Eur J Radiol 2009;70:475‑80.
10. Sempere AP, Villaverde FJ, Martinez‑MenCndez B, Cabeza C, Peiia P, Tejerina JA. First seizure in adults: A prospective study from the emergency department. Acta Neurol Scand 1992;86:134‑8.
11. Schoenenberger RA, Heim SM. Indication for computed tomography of the brain in patients with first uncomplicated generalised seizure. BMJ 1994;309:986‑9.
12. Hopkins A, Garman A, Clarke C. The first seizure in adult life. Value of clinical features, electroencephalography, and
computerised tomographic scanning in prediction of seizure recurrence. Lancet 1988;1:721‑6.
13. Silverstein AM, Alexander JA. Acute postictal cerebral imaging. AJNR Am J Neuroradiol 1998;19:1485‑8.
14. Bukte Y, Kemaloglu S, Nazaroglu H, Ozkan U, Ceviz A, Simsek M. Cerebral hydatid disease: CT and MR imaging findings. Swiss
Med Wkly 2004;134:459‑67.
15. Jayakumar PN, Taly AB, Mohan PK. Transient computerised tomographic abnormalities following partial seizures. Acta Neurol
Scand 1985;72:26‑9.
16. Young AC, Costanzi JB, Mohr PD, Forbes WS. Is routine computerised axial tomography in epilepsy worth while? Lancet 1982; 2:1446‑7.
17. Puri V, Gupta RK. Magnetic resonance imaging evaluation of focal computed tomography abnormality in epilepsy. Epilepsia
1991;32:460‑6.
18. Luhdorf K, Jensen LK, Plesner AK. Etiology of seizures in the elderly. Epilepsia 1986;27:458‑63.
19. Hsieh DT, Chang T, Tsuchida TN, Vezina LG, Vanderver A, Siedel J, et al. New‑onset afebrile seizures in infants: role of neuroimaging. Neurology 2010;74:150‑6.
20. Bhargava S, Tandon PN. Intracranial tuberculoma: A CT study. Br J Radiol 1980;53:935‑45.
21. Kumar R, Kumar A, Kohli N Pant MC, Govil YC, Sharma B. Ring or disc like enhancing lesions in partial epilepsy in India. J Trop
Pediatr 1990;36:131‑4.
22. Wadia RS, Makhale CN, Kelker AV, Grant KB. Focal epilepsy in India with special reference to lesions showing ring or disc like enhancement on contrast computed tomography. J Neurol Neurosurg Psychiatry 1987;50:1298‑301.
23. Sethi PK, Kumar BR, Madam VS, Mohan V. Appearing and disappearing CT scan abnormalities and seizures. J Neurol Neurosurg Psychiatry 1985;48:866‑9.