

Opaque Hemithorax: Clinical, Histological and Radiological Assessment of 30 Cases at a Tertiary Care Hospital- A Preliminary Study
Article Sidebar
Views | PDF/EPUB Downloads:
307
/ 84
/ 38
Main Article Content
Abstract
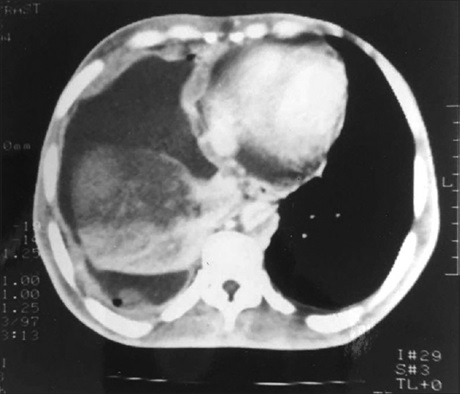
Background: Whitening out of half of the lung field on a chest X‑ray is known as opacification of a hemithorax, and its presence usually indicates a significant disease in a patient. This study was done with an aim of finding different etiologies as the cause of complete opacification of a hemithorax on chest radiograph.
Materials and Methods: An observational cross‑sectional study of patients whose chest radiograph had opaque hemithorax was included and after clinical laboratory and advanced radiological ‑ ultrasonography (USG) and computed tomography investigation of these patients the diagnosis responsible for the complete opacification of half the lung field in chest X‑ray was recorded.
Results: Atotal of 30 patients (23 males and 7 females) were enrolled for the study. Out of the 30 patients, 17 involved the left while 13 involved the right hemithorax. Fifteen patients had clear pleural effusion, 13 patients had mass with pleural
effusion and 2 patients were postpneumonectomy cases. Mediastinal shift to contralateral side was seen in 18 out of 30 patients having opaque hemithorax. Eleven patients have biochemical features of tuberculosis. All 13 patients with mass and effusion were confirmed to have malignancy on histology. USG could detect malignancy in only ten cases. Chest pain was most frequent symptom and smoking or tobacco habit was associated with 14 cases.
Conclusion: Plain pleural effusion was the most common etiology of opaque hemithorax in our study followed by mass with effusion. Among other rarer causes, only pneumonectomy was seen. For other rare causes that may present as opaque hemithorax larger study may be done.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Bharty S, Prakash B, Agarwal M, Bhatnagar A. Opaque hemithorax: Re‑visiting the causes. Internet J Pulm Med 2013;14:1‑5.
2. Bhagat R, Panchal N, Shah A. Pulmonary aplasia: A CT appearance. Indian Pediatr 1992;29:1410‑2.
3. Kawashima A, Libshitz HI. Malignant pleural mesothelioma: CT manifestations in 50 cases. AJR Am J Roentgenol 1990;155:965‑9.
4. Yilmaz UM, Utkaner G, Yalniz E, Kumcuoglu Z. Computed tomographic findings of environmental asbestos‑related malignant
pleural mesothelioma. Respirology 1998;3:33‑8.
5. Porcel JM, Vives M. Etiology and pleural fluid characteristics of large and massive effusions. Chest 2003;124:978‑83.
6. Ahmad A, Khan AZ, Bilal A, Rabbi F, Ahmad Y. Diagnostic outcome of large and massive Pleural effusion. Pak J Chest Med 2008; 14:4‑10.
7. Light RW, Erozan YS, Ball WC Jr. Cells in pleural fluid. Their value in differential diagnosis. Arch Intern Med 1973;132:854‑60.
8. Marel M, Zrustová M, Stasný B, Light RW. The incidence of pleural effusion in a well‑defined region. Epidemiologic study in central
Bohemia. Chest 1993;104:1486‑9.
9. Johnston WW. The malignant pleural effusion. A review of cytopathologic diagnoses of 584 specimens from 472 consecutive
patients. Cancer 1985;56:905‑9.
10. Naito T, Satoh H, Ishikawa H, Yamashita YT, Kamma H, Takahashi H, et al. Pleural effusion as a significant prognostic factor
in non‑small cell lung cancer. Anticancer Res 1997;17:4743‑6.
11. Chernow B, Sahn SA. Carcinomatous involvement of the pleura: An analysis of 96 patients. Am J Med 1977;63:695‑702.