

Multiple brown tumors: unusual presentation of parathyroid carcinoma
Article Sidebar
Views | PDF/EPUB Downloads:
345
/ 46
/ 40
Main Article Content
Abstract
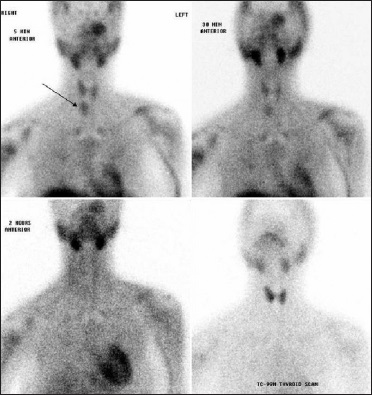
Brown tumors represent the terminal stage of the remodeling process during hyperparathyroidism, and it is a rare clinical presentation of primary hyperparathyroidism. Parathyroid carcinoma is even more rare cause of primary hyperparathyroidism. This is a report of a multiple brown tumor caused by primary hyperparathyroidism secondary to parathyroid carcinoma. A 41-year-old woman, who was presented with a generalized bony pain and pathological fracture of left humerus. X-ray demonstrated lytic lesion in bilateral humerus and left ulna. Laboratory investigations showed hypercalcemia and hypophosphatemia with elevated parathyroid hormone level. Ultrasonography did not reveal any parathyroid lesion, whereas radionuclide Sestamibi scan delineated a focus of abnormal tracer uptake in the lower pole region of right lobe of thyroid, left maxilla, bilateral humerus, and left clavicle. She underwent right inferior
parathyroidectomy, right hemithyroidectomy and central node dissection. Histological diagnosis confirmed parathyroid carcinoma. The rarity and the interesting clinical presentation of such association are discussed.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Di Danelle N, Condò S, Ferrannini M, Bertoli M, Rovella V, Di Renzo L, et al. Brown tumor in a patient with secondary hyperparathyroidism resistant to medical therapy: Case report on successful treatment after subtotal parathyroidectomy. Int J
Endocrinol 2009;2009:827652.
2. Thompson NW, Eckhauser FE, Harness JK. The anatomy of primary hyperparathyroidism. Surgery 1982;92:814‑21.
3. Hruska K. New concepts in renal osteodystrophy. Nephrol Dial Transplant 1998;13:2755‑60.
4. Takeshita T, Takeshita K, Abe S, Takami H, Imamura T, Furui S. Brown tumor with fluid‑fluid levels in a patient with primary
hyperparathyroidism: Radiological findings. Radiat Med 2006;24:631‑4.
5. Takeshita T, Tanaka H, Harasawa A, Kaminaga T, Imamura T, Furui S. Brown tumor of the sphenoid sinus in a patient with
secondary hyperparathyroidism: CT and MR imaging findings. Radiat Med 2004;22:265‑8.
6. Gayed IW, Elshazly SM, Vang RS, Barron BJ, Lamki LM. Technetium‑99m sestamibi uptake in a maxillary brown tumor.
Clin Nucl Med 2001;26:65‑7.
7. Tziakouri C, Eracleous E, Skannavis S, Pierides A, Symeonides P, Gourtsoyiannis N. Value of ultrasonography, CT and MR imaging
in the diagnosis of primary hyperparathyroidism. Acta Radiol 1996;37:720‑6.
8. Gotway MB, Leung JW, Gooding GA, Litt HI, Reddy GP, Morita ET, et al. Hyperfunctioning parathyroid tissue: Spectrum of appearances on noninvasive imaging. AJR Am J Roentgenol 2002;179:495‑502.
9. Chiu ML, Kronauge IF, Piwnica‑Worms D. Effect of mitochondrial and plasma membrane potentials on accumulation of hexakis (2‑methoxyisobutylisonitrile) technetium (I) in cultured mouse fibroblasts. J Nucl Med 1990;31:1646‑53.
10. Jebasingh F, Jacob JJ, Shah A, Paul TV, Seshadri MS. Bilateral maxillary brown tumors as the first presentation of primary
hyperparathyroidism. Oral Maxillofac Surg 2008;12:97‑100.
11. Kaya RA, Cavuşoğlu H, Tanik C, Kahyaoğlu O, Dilbaz S, Tuncer C, et al. Spinal cord compression caused by a brown tumor at the
cervicothoracic junction. Spine J 2007;7:728‑32.