

Baseline chest radiographic features among antiretroviral therapy naïve human immuno-deficiency virus positive children in a pediatric care program
Article Sidebar
Views | PDF/EPUB Downloads:
363
/ 40
/ 51
Main Article Content
Abstract
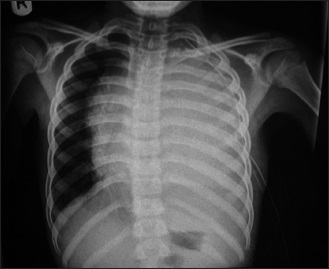
Background: Pulmonary diseases are commonly seen in children with HIV infection, and their etiology is often unclear. The radiological appearances of these conditions are often non-specific. Conventional radiographs play an important role in the management of chest conditions especially in resource poor settings.
Objective: This retrospective study was carried out to determine the chest radiographic pattern in children with HIV infection.
Materials and Methods: The baseline chest X-ray of 150 HIV-positive but antiretroviral drug naïve children were analyzed between July 2008 and December 2009 at the University College Hospital in Ibadan, south-west Nigeria. All children were screened for tuberculosis (TB) by one or combination of mantoux, acid-fast Bacilli (AFB) sputum, and erythrocyte
sedimentation rate. The CD4 count was also taken as part of baseline laboratory test. Chi-squared test was used to determine association between the pattern of chest X-ray findings, and sex, age, and CD4 counts.
Results: The mean age of the study group was 51.6 months, with children older than 5 years dominating and there was no statistical difference in the sex distribution. A total of 115 children (76.7%) had abnormal chest X-ray, with lymphadenopathy accounting for 45.3% followed by parenchymal lesions with 37.3%, miliary shadows, and cavities accounted for 6.7% and 2.6%, respectively. Cavities were found to be common in patient who tested positive to AFB than AFB-negative patients. Other findings like reticulonodular or diffuse patterns, lymphadenopathy, pleural effusion, or soft tissue swelling were also commoner in the AFB-positive patients. The CD4 count was available for 42% of the patient and there was no significant association between the chest radiographic changes and the CD4 count.
Conclusion: Definitive diagnosis of pulmonary disease might be difficult based on chest X-ray alone, however, chest X-ray is a basic radiological test and almost the easiest to perform in both resource poor or rich setting and it is still recommended that routine chest X-ray should remain part of investigation of HIV-positive children to serve as adjunct to other investigations in early detection of TB.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Federal Ministry of Health. Focus on AIDS. Niger Bull Epidemiol1992;2:1‑8.
2. UNAIDS. Report on the global HIV/AIDS epidemics 2008. Geneva: UNAIDS; 2008. p. 11‑356.
3. Theron S, Andronikou S, George R, du Plessis J, Goussard P, Hayes M, et al. Non‑infective pulmonary disease in HIV‑positive
children. Pediatr Radiol 2009;39:555‑64.
4. George R, Andronikou S, Theron S, du Plessis J, Hayes M, Goussard P, et al. Pulmonary infections in HIV‑positive children. Pediatr Radiol 2009;39:545‑54.
5. Dramowski A, Morsheimer MM, Frigati L, Schaaf HS, Rabie H, Sorour G, et al. Radiology services for children in HIV‑ and TB‑endemic regions: Scope for greater collaboration between radiologists and clinicians caring for children. Pediatr Radiol
2009;39:541‑4.
6. Pitcher RD, Goddard E, Hendricks M, Lawrenson J. Chest radiographic pulmonary changes reflecting extrapulmonary involvement in paediatric HIV disease. Pediatr Radiol 2009;39:565‑8.
7. Castañer E, Gallardo X, Mata JM, Esteba L. Radiologic approach to the diagnosis of infectious pulmonary diseases in patients infected with the human immunodeficiency virus. Eur J Radiol 2004;51:114‑29.
8. Oh YW, Effmann EL, Godwin JD. Pulmonary infections in immunocompromised hosts: The importance of correlating the
conventional radiologic appearance with the clinical setting. Radiology 2000;217:647‑56.
9. Owens CM, Allan R, Thomas K, Evans J, Stevens J. Pictorial review: The radiological spectrum of vertically‑acquired HIV infection. Br J Radiol 1996;69:777‑82.
10. McAdams HP, Erasmus J, Winter JA. Radiologic manifestations of pulmonary tuberculosis. Radiol Clin North Am 1995;33:655‑78.
11. Kang EY, Staples CA, McGuinness G, Primack SL, Müller NL. Detection and differential diagnosis of pulmonary infections and
tumors in patients with AIDS: Value of chest radiography versus CT. AJR Am J Roentgenol 1996;166:15‑9.
12. King IJ, Padley SP. Imaging of the thorax in AIDS. Imaging 2002;14:60‑76.
13. Balogun TM, Sagoe A, Taiwo T. HIV seroprevalence among children outpatients in Lagos Hospital, Nigeria. Niger Med Pract 2008; 54:75‑9.
14. Bugaje MA, Aikhionbare HA. Paediatrics HIV/AIDS seen at Ahamadu Bello University Teaching Hospital Zaria, Nigeria. Ann Afr Med 2006;5:73‑7.
15. Shah I, Katira B. Seroprevalence of HIV infection in hospitalized paediatric patients at a tertiary care centre in western India. HIV
Med 2007;8:265‑6.
16. Lodha R, Upadhyay A, Kapoor V, Kabra SK. Clinical profile and natural history of children with HIV infection. Indian J Pediatr 2006;73:201‑4.
17. Shah I. Age related clinical manifestations of HIV infection in Indian children. J Trop Pediatr 2005;51:300‑3.
18. Daga SR, Verma B, Gosavi DV. HIV infection in children: Indian experience. Indian Pediatr 1999;36:1250‑3.
19. Ugochukwu EF. Clinical spectrum of paediatric HIV in Nnewi, Nigeria. West Afr J Med 2006;25:10‑4.
20. Akolo C, Ukoli CO, Ladep GN, Idoko JA. The clinical features of HIV/AIDS at presentation at the Jos University Teaching Hospital.
Niger J Med 2008;17:83‑7.
21. Okechukwu AA, Gambo D, Okechukwu OI. The clinical features of paediatric HIV/AIDS at presentation at the University of Abuja
Teaching Hospital, Gwagwalada. Niger J Med 2008;17:433‑8.
22. Franquet T. Respiratory infection in the AIDS and immunocompromised patient. Eur Radiol 2004;14:E21‑33.
23. Kisembo HN, Kawooya MG, Zirembuzi G, Okwera A. Serial chest radiographs in the management of children with a clinical
suspicion of pulmonary tuberculosis. J Trop Pediatr 2001;47:276‑83.
24. Haramati LB, Jenny‑Avital ER. Approach to the diagnosis of pulmonary disease in patients infected with the human
immunodeficiency virus. J Thorac Imaging 1998;13:247‑60.
25. Marquis JR, Berman CZ, DiCarlo F, Oleske JM. Radiographic patterns of PLH/LIP in HIV positive children. Pediatr Radiol 1993; 23:328‑30.
26. Milković D, Richter D, Zoricić‑Letoja I, Raos M, Koncul I. Chest radiography findings in primary pulmonary tuberculosis in children. Coll Antropol 2005;29:271‑6.
27. Jones BE, Ryu R, Yang Z, Cave MD, Pogoda JM, Otaya M, et al. Chest radiographic findings in patients with tuberculosis with recent or remote infection. Am J Respir Crit Care Med 1997;156:1270‑3.
28. Brahmbhatt H, Kigozi G, Wabwire‑Mangen F, Serwadda D, Lutalo T, Nalugoda F, et al. Mortality in HIV‑infected and uninfected children of HIV‑infected and uninfected mothers in rural Uganda. J Acquir Immune Defic Syndr 2006;41:504‑8.
29. Andronikou S, Welman CJ, Kader E. The CT features of abdominal tuberculosis in children. Pediatr Radiol 2002;32:75‑81.
30. Swaminathan S. Tuberculosis in HIV‑infected children. Paediatr Respir Rev 2004;5:225‑30.
31. Iriso R, Mudido PM, Karamagi C, Whalen C. The diagnosis of childhood tuberculosis in an HIV‑endemic setting and the use of
induced sputum. Int J Tuberc Lung Dis 2005;97:716‑26.
32. Temiye EO, Akinsulie AO, Ezeaka CV, Adetifa IM, Iroha EO, Grange AO, et al. Constraints and prospects in the management of pediatric HIV/AIDS. J Natl Med Assoc 2006;98:1252‑9.
33. Nyamande K, Lalloo UG, Vawda F. Comparison of plain chest radiography and high‑resolution CT in human immunodeficiency
virus infected patients with community‑acquired pneumonia: A sub‑Saharan Africa study. Br J Radiol 2007;80:302‑6.
34. Marais BJ, Graham SM, Cotton MF, Beyers N. Diagnostic and management challenges for childhood tuberculosis in the era of
HIV. J Infect Dis 2007;196:S76‑85.