

Computed Tomographic Assessment in Deep space Infections of Odontogenic Origin
Article Sidebar
Views | PDF/EPUB Downloads:
338
/ 78
/ 32
Main Article Content
Abstract
Background/Aim: The objective of the article is to investigate the pathways of spread of odontogenic infection in the facial and neck spaces and to determine the accuracy of contrast enhanced computed tomography (CT) in diagnosing deep neck space infections.
Study Design/Materials and Methods: Contrast enhanced CT scans of 27 patients with extensive spread of odontogenic infection into the facial and neck spaces were analyzed to document the pathways of spread.
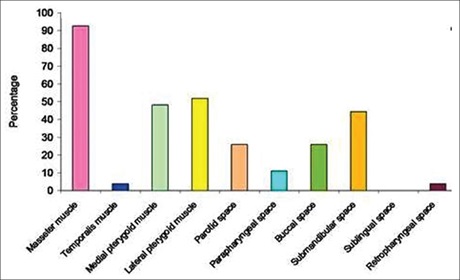
Results: The results of the study indicated that the masseter space was the most commonly involved space followed by the pterygoids (both lateral and medial) and a different spread (other than medial pterygoids) to the parapharyngeal space has been proposed. Odontogenic infections from the mandible spread in two different ways. It first spreads upward, into the masseter and/or medial pterygoid muscles in the masticator space, and downward, into the sublingual and/ or submandibular spaces, and then spreads into the spaces or muscles adjacent to one or more of these locations. Infections from the masseter muscle spreads into the parotid space to involve the temporalis and lateral pterygoid muscles. Infections from the medial pterygoid muscle spread into the parapharyngeal space to involve the lateral pterygoid muscle. Infections in the maxilla do not spread downward; instead, they tend to spread upward and superficially into the buccal space.
Conclusion: CT is useful in depicting the exact site and extent of infection and in planning the treatment of extensive odontogenic infection, which can be life threatening when therapy is ineffective.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Yonetsu K, Izumi M, Nakamura T. Deep Facial Infections of Odontogenic Origin: CT Assessment of Pathways of Space Involvement. AJNR Am J Neuroradiol 1998;19:123‑8.
2. Ohshima A, Ariji Y, Goto M, Izumi M, Naitoh M, Kurita K, et al. Anatomical considerations for the spread of odontogenic infection
originating from the pericoronitis of impacted mandibular third molar: Computed tomographic analyses. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 2004;98:589‑97.
3. Cmejrek RC, Coticchia JM, Arnold JE. Presentation, diagnosis, and management of deep‑neck abscesses in Infants. Arch OtolaryngolHead Neck Surg 2002;128:1361‑4.
4. Flynn TR, Shanti RM, Levi MH, Adamo AK, Kraut RA, Trieger N. Severe Odontogenic Infections Part 1: Prospective Report. J Oral
Maxillofac Surg 2006;64:1093‑103.
5. Jankowska B, SalamiA, Cordone G, Ottoboni S, Mora R. Deep neck space infections. Int Congr Ser 2003;1240:1497‑500.
6. Bridgeman A, Wiesenfeld D, Hellyar A, Sheldon W. Major maxillofacial infections: An evaluation of 107 cases. Aust Dent J 1995; 40:281‑8.
7. Chang L, Chi H, Chiu NC, Huang FY, Lee KS. Deep Neck Infections in Different Age Groups of Children. J Microbiol Immunol Infect
2010;43:47‑52.
8. Obayashi N, Ariji Y, Goto M, Izumi M, Naitoh M, Kurita K, et al. Spread of odontogenic infection originating in the maxillary teeth:
Computerized tomographic assessment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:223‑31.
9. Miller WD, Furst IM, Sàndor GK, Keller MA. A prospective, blinded comparison of clinical examination and computed tomography in deep neck infections. Laryngoscope 1999;109:1873‑9.
10. Nagy M, Backstrom J. Comparison of the sensitivity of lateral neck radiographs and computed tomography scanning in pediatric
deep‑neck infections. Laryngoscope 1999;109:775‑9.