

Preliminary Result on The Use of Bone Scan and Plain X-rays in the Evaluation of Bone Metastasis From Breast Cancer in a Tertiary Institution: A Study of 30 Patients
Article Sidebar
Views | PDF/EPUB Downloads:
249
/ 26
Main Article Content
Abstract
Title: Preliminary result on the use of bone scan and plain x-rays in the evaluation of bone metastases from breast cancer in a tertiary institution: a study of 30 patients.
Background: Bone scan is superior to plain x-rays in diagnosing early bone metastasis in management of cancer patients be made known and exploited, so as to manage such cases before irreversible damages are caused.
Objective: To evaluate the role of bone scan and plain x-rays in the management of bone metastasis from breast cancer as seen in a tertiary referral center.
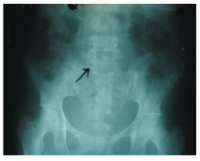
Materials and Methods: Between January to December 2000, 30 consecutive patients with histologically confirmed breast cancer and bone pain presenting for the first time in the clinic or attending follow up clinic, were studied. All the patients were investigated with bone scan and x-rays of relevant bones at first presentation of pain, irrespective of duration of symptoms. Study was conducted at Nuclear Medicine, Oncology and Radiotherapy Institute (NORI), Islamabad Pakistan. Relevant patients' data on details of disease since onset were accessed from records.
Results: Six patients had painful bone metastases for 3 months; fourteen had pain for 4 6 months; two had pain for 7.9 months; three had pain for 10 12 months; and five had pain for more than 12 months prior to treatment with radiotherapy. Of the twenty patients presenting with pain for 6 months and below, all had radiological confirmation of bone metastasis on bone scan and only one had radiological confirmation of bone metastasis with plain x-rays at time of initial investigation. All the patients having bone pain for at least 9 months had confirmation of bone metastasis with plain x-rays at initial investigations. All the patients with evidence of bone metastasis on bone scan were confirmed with plain x-rays after at least 9 months of onset of bone pain.
Conclusion: Although the number of patients was few, waiting for 9 months for radiological confirmation of bone metastasis will definitely have adverse effects on the quality of life of patients, performance status and chance of controlling the symptoms for a long time. Therefore, bone scan should be in the initial staging investigations of all patients. Facility for bone scan and nuclear imaging should be made widely available in tertiary institutions including those in resource poor countries.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Ketika, KK. The pattern of metastases in Nigerian breast patients. Clinical Oncology, 1996,37-563-565
2. Galasko CSB. The anatomy and pathways of skeletal metastases, In: Weiss L., Cälbert AH (eds): Bone Metastasis. Boston, GK Hall, 1961, pp 49 63.
3. Body J. Clinical trials in Metastatic bevast cancer to bone: past-present-future. Can Oncol 1995 Dec; 5 Suppl 1: 16-27 Reviww.
4. Adewuyi SA, Shittu SO, Rafmdadi AH Sociodemographic and Clinicopathologic Characterization of Cervical Canor in Northern Nigeria Eur. J. Gynaec. Oncol (ECO). 2008; vol 29(1):61-64.
5. Adewuyi SA, Chom ND, Hamera M. Pattern of Skeletal metastases from breast cancer in an Asian population. The Nigerian Journal of Surgical Research. 2006; vol. 8:128-131
6. Cosfield E, Alavi A, Kneeland l. Comparison of radionuclide borw scans and magnetic resemance imaging in detecting spinal. metastases. J Nucl Med 1993, 34:2191
7. Pomerana St. Pretorius HT, Ramingh PS Hone Scintigraphy and multimodalities imaging in bone neoplasia strategies for imaging in the new health care climate. Semin Nucl Med 1994; 24:188
8. Berruti A, Dolitotti 1, Corzegno G. Torta M. Tampellini M, Tucci M, Cerutti 5, Prezet MM, Stivanelle M. Sacchetto G. Angeli A. Differential patterns of bome turnover in relation to bone pain and disease extent in bone in cancer patients with skeletal metastases. Clinical Chemistry 1999, 45:1240
9. Stephen Chapman, Richard Nakielny: Aids to Radiological Differential Diagnosis. 3 Edition, 1995, London, W. IB Saunders company limited
10. Kagan RA, Stockel R. J., Basset L. W. & Gold R. H. Radiologic contributions to cancer management. Bone metastases. Am. J. Roentgenol. 1986, 147:305-312
11. Yoneda T, Sasaki A, Mandy GR: Osteolytic bone metastases in breast cancer. Breast Cancer Res Treat 1994, 32:73-84.
12. Body J. Metastatic bone disease: Clinical arsd therapeutic aspects. Воно 1992, 13557-562.
13. Thrall J. H., Ellis B. 1. Skeletal metastases Radiol. Clin North Am. 1987, 251155-1170.
14. Orr FW, Kostenuik P, Sanchez-Sweatman OH, Singh G. Mechanisans involved in the metastases of cancer to bone. Breast Cancer Res Treat 1993, 25:151
15. Potterson H. Gillespy T, Hamlin Dj et al Primary musculoskeletal tumora examirsation with MR imaging compared with conventional modalities, Radiology 1967: 164:237-241
16. Murray RO, Jacobson HG. The Radiology of skeletal disorder. 3 Edition. Churchill Livingstone, Edinburgh 1992: 132-139