

A case of renal artery embolization for Grade 5 renal injury, usually reserved for surgery
Article Sidebar
Views | PDF/EPUB Downloads:
389
/ 60
/ 42
Main Article Content
Abstract
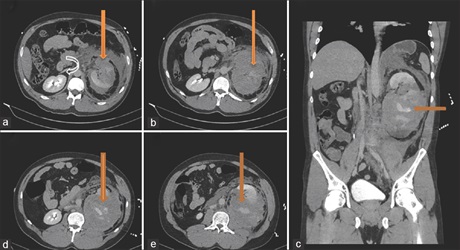
Kidney trauma occurs in approximately 1%–5% of all traumas with the male preponderance. The consequences of blunt renal trauma range from a simple contusion or renal hematoma to complete shattering of the organ or avulsion of the vascular pedicle. Recently, there is more focus on conservative management as newer techniques evolve and its currently the preferred approach to most renal injuries; however, surgery is the main treatment modality for avulsion of the renal pelvis, injuries to the vascular pedicle, and life-threatening hemodynamic instability. Renal artery embolization is a minimally invasive procedure used in the management of many disease conditions and also to control hemorrhage. We report of a Grade 5 renal injury with hemodynamic instability managed with renal artery embolization which otherwise would have been managed with surgery. A 33-year-old presented with Grade 5 left renal
injury and hemodynamic instability after a fall. Computed tomography of the abdomen after resuscitation showed shattered left kidney with disruption of the renal hilum and features suggestive of active bleeding. Due to the hypovolemic nature of the patient, embolization of the renal artery was requested. With anesthetic support and antibiotic cover, the right common femoral artery was punctured and a 5 French sheath inserted. Both left renal arteries were selectively catheterized and embolized to stasis with coils. An Angio-Seal device was deployed in the groin and no immediate complications seen. The patient was discharged few days after. This case report shows that Grade 5 renal artery can also be managed through a minimal invasive procedure to reduce the length of time at the hospital and also reduce the metabolic response of the patient.
Downloads
Article Details
Section

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
How to Cite
References
1. Bent C, Iyngkaran T, Power N, Matson M, Hajdinjak T, Buchholz N, et al. Urological injuries following trauma. Clin Radiol 2008;63:1361‑71.
2. Martínez‑Piñeiro L, Djakovic N, Plas E, Mor Y, Santucci RA, Serafetinidis E, et al. EAU guidelines on urethral trauma. Eur Urol 2010;57:791‑803.
3. Santucci RA. High‑grade renal injury: Non‑operative management of urinary extravasation and prediction of long‑term outcomes. BJU Int
2013;111:E256.
4. Davis KA, Reed RL 2nd, Santaniello J, Abodeely A, Esposito TJ, Poulakidas SJ, et al. Predictors of the need for nephrectomy after renal trauma. J Trauma 2006;60:164‑9.
5. Santucci RA, McAninch JW, Safir M, Mario LA, Service S, Segal MR, et al. Validation of the American Association for the Surgery of Trauma
organ injury severity scale for the kidney. J Trauma 2001;50:195‑200.
6. Mee SL, McAninch JW, Robinson AL, Auerbach PS, Carroll PR. Radiographic assessment of renal trauma: A 10‑year prospective study of patient selection. J Urol 1989;141:1095‑8.
7. Wessells H, Suh D, Porter JR, Rivara F, MacKenzie EJ, Jurkovich GJ, et al. Renal injury and operative management in the United States: Results of a population‑based study. J Trauma 2003;54:423‑30.
8. Kuo RL, Eachempati SR, Makhuli MJ, Reed RL 2nd. Factors affecting management and outcome in blunt renal injury. World J Surg 2002; 26:416‑9.
9. Heyns CF, de Klerk DP, de Kock ML. Stab wounds associated with hematuria – A review of 67 cases. J Urol 1983;130:228‑31.
10. Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, et al. Organ injury scaling: Spleen, liver, and kidney. J Trauma 1989;29:1664‑6.
11. Buckley JC, McAninch JW. Revision of current American Association for the Surgery of trauma renal injury grading system. J Trauma 2011; 70:35‑7.
12. Santucci RA, Wessells H, Bartsch G, Descotes J, Heyns CF, McAninch JW, et al. Evaluation and management of renal injuries: Consensus statement of the renal trauma subcommittee. BJU Int 2004;93:937‑54.
13. Bryk DJ, Zhao LC. Guideline of guidelines: A review of urological trauma guidelines. BJU Int 2016;117:226‑34.
14. Santucci RA, McAninch JW. Diagnosis and management of renal trauma: Past, present, and future. J Am Coll Surg 2000;191:443‑51.
15. Breyer BN, McAninch JW, Elliott SP, Master VA. Minimally invasive endovascular techniques to treat acute renal hemorrhage. J Urol
2008;179:2248‑52.
16. Robert M, Drianno N, Muir G, Delbos O, Guiter J. Management of major blunt renal lacerations: Surgical or nonoperative approach? Eur
Urol 1996;30:335‑9.
17. Bauer JR, Ray CE. Transcatheter arterial embolization in the trauma patient: A review. Semin Intervent Radiol 2004;21:11‑22.